
CO-GRAFT OF ACELLULAR DERMAL MATRIX AND AUTOGENOUS MICROSKIN IN A CHILD WITH EXTENSIVE BURNS
SUMMARY. A 6-yr-old boy was the victim of a burns accident in a public bathhouse. The burns involved the face, neck, upper and lower extremities, anterior and posterior trunk, and both buttocks, covering 72% of the total body surface area (TBSA). The lesions in the lower extremities and parts of the right upper extremity were deep partial-thickness, comprising 40% TBSA. On day 5 post-burn, the lesions in both lower extremities were excised to the extent of the fascia under general anaesthesia. Meshed J1 Jayya Acellular Dermis®, a kind of acellular allodermal (ADM) matrix, was then placed on the left knee joint. The right knee joint served as control. The wounds in both lower extremities were then overlaid with microskin autografting. At 19 days post-application, the lesions in both lower extremities had almost completely resurfaced. Follow-up at six months revealed well-healed and stable skin of acellular ADM and microskin autografts on the left knee. However, the skin of the right knee was unstable and there was a chronic residual ulcer. Both legs showed some significant hypertrophic scars. The left knee joint (acellular ADM grafted site) showed mild contractures, while the right knee joint developed a significant contracture. The “skin” of the co-graft covered site appeared thicker and more elastic. The movement range of the left knee joint was much larger than that of the right knee joint. These results suggest that co-graft of acellular dermal matrix and autogenous microskin may be an effective way to repair this functional site in children with extensive burns and to improve the functional and cosmetic results.
Introduction
Microskin grafting has proved to be an effective method for the treatment of extensive burns in which the area of available donor skin is inadequate.1 In this method, a piece of thin split-thickness autogenous skin (0.15-0.30 mm in thickness) is harvested and minced into tiny particles for grafting. Owing to the lack of dermis, the healed wound always has a poor functional and cosmetic result.2 A chronic ulcer and a severe hypertrophic scar often develop. In the joint area, contracture of the scar always confines movement. To improve the overall cosmetic and functional outcome of microskin autograft, a co-graft of allodermal matrix (ADM) and autogenous microskin was utilized both in animals and in adult patients.2-4 The co-graft skins had a very elastic and smooth texture compared with traditional microskin autografts, showing less cicatrization and ulceration.3 Here we report on a successful application of co-graft of acellular ADM and autogenous microskin in a 6-yr-old child with extensive burns.Case report
A 6-yr-old boy was the victim of an accident that occurred in a public bathhouse on 31 January 2005, when he fell into the boiling-water pool as he walked along the edge of the pool. The patient sustained burns due to boiling water. After being removed from the source of his injury, the patient was transported to a local medical unit 15 min post-burn. Topical moist exposed burn ointment (MEBO) was applied. After a period of 8 h, the patient was transferred to our burns centre. During transit, the patient was resuscitated with 625 ml liquid, including 300 ml Ringer’s lactated fluid, 125 ml sodium bicarbonate, and 200 ml low molecular weight dextran. Besides the intravenous fluid, he drank a total of 500 ml plain boiled water.On admission, the patient was found to be in a state of hypovolaemic shock: he was thirsty, his skin was cool and white, his pulse weak, and capillary refill was delayed. The burns involved the face, neck, upper and lower extremities, anterior and posterior trunk, and both buttocks, covering 72% of his total body surface area (TBSA) (Fig. 1).
|

The wounds in both lower extremities and parts of the right upper extremity were deep partial-thickness, comprising 40% TBSA (Fig. 2); the rest of the wounds were superficial partial-thickness. Prompt venotomy was performed to establish intravenous access. Resuscitation with Ringer’s lactated fluid and plasma was given and adjusted to a maintenance level of adequate urine output and haemodynamics. Haemodynamic stability was achieved and the patient’s thirst was relieved following fluid infusion and debridement of the injured areas. Silver sulphadiazine was applied to the wounds and covered with dry dressings. Fluid input in the first 24 h totalled 3350 ml, achieving a diuresis of 40-50 ml per h. The patient was treated with 2100 ml fluid and his urine output was 1540 ml in the second 24 h.
On day 5 post-burn, the wounds in both lower extremities were excised to the extent of the fascia under general anaesthesia (Fig. 3).
|

|

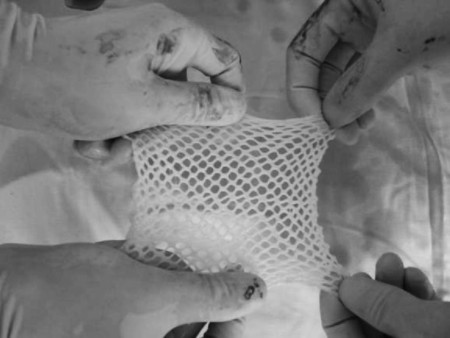
Meshed J1 Jayya Acellular Dermis® (Beijing Jayya Life Tissue Engineering Co., Ltd, Beijing, China), a kind of acellular ADM like Alloderm®, was then placed in the haemostatic tissue bed of the left knee joint and secured by suture (Fig. 4). The right knee joint served as control (Fig. 5).
|
|

The wounds in both lower extremities were then overlaid with microskin autografting, which was performed as described by Zhang with slight modifications.5 In brief, thin split-thickness autogenous skin (3% TBSA) was harvested using a compressed-air-powered dermatome (Zimmer Corp., Denver, OH) from the scalp of the patient as needed at a depth of 0.2 mm, cut into tiny pieces smaller than 1 mm3 using a pair of fine scissors, and then immersed in normal saline. The minced skin gradually floated with the epithelial side upwards. The floating particles of skin were removed from the saline and evenly spread on a piece of silk cloth with a spoon, keeping the epithelial side upwards. A large sheet of homograft was taken out of a supra-low temperature refrigerator and thawed in normal saline at 37 °C, after which some holes were made in it using a scalpel for exudation drainage. The large sheet of homograft was placed over the microskin grafts on the silk cloth, the dermal side of the homograft making contact with the epithelial side of the micrografts. The homograft and the silk cloth were turned over together and the cloth was carefully removed, leaving the micrografts in contact with the homograft (Fig. 6).
|
This time the microskin grafts were also turned over with the dermal side up (the same as the homograft). The prepared homograft-autograft was transplanted onto the excised burn wound in both lower extremities and secured in sheets to the wound margin using a combination of staples and unabsorbable sutures (Figs. 7, 8).
|

|

Gentamycin- impregnated Vaseline gauze, followed by an additional layer of outer bulk gauze wrap, completed the dressings, which remained intact for seven days. On day 6 post-operation, the intravenous catheter was removed and its bacterial culture was found to be negative. The outer dressing was first changed on day 7 after grafting. The success of the initial graft take was determined at day 10, when all dressings were removed (Fig. 9).
|

At 19 days post-application, the wounds in both lower extremities had almost completely resurfaced (Fig. 10).
|

The remaining wounds were dressed with silver sulphadiazine 1% and changed every two days. On day 68 post-burn, the residual 3% TBSA defects were covered with split-thickness autografts. After this procedure, all the wounds were closed and the patient was discharged on day 79 after the injury.
Follow-up at six months revealed well-healed and stable skin of acellular ADM and microskin autografts on the left knee. However, the skin of right knee was unstable and there was a chronic and residual ulcer with a diameter of 1 cm (Fig. 11).
|

Both legs showed some significant hypertrophic scars. The left knee joint (acellular ADM-grafted site) showed mild contractures, while the right knee joint, not covered with acellular ADM but directly with traditional microskin autografts, developed significant contracture (Fig. 12).
|

The “skin” of the co-graft-covered site appeared thicker and more elastic. The movement range of the left knee joint was much larger than that of the right knee joint.
Discussion
It is always a challenging problem for a burn surgeon to be confronted with a patient with extensive full-thickness burns and insufficient viable skin available for autografting. The Integra Dermal Regeneration Template®, an artificial skin system, has been demonstrated to provide early wound coverage and has been used effectively to treat deep excised wounds of the skin.# However, the use of Integra® is limited in the developed countries owing to its high expense, while in the developing countries such as China very few patients can afford it.In 1986, Zhang and his colleagues first described a new technique of skin graft called the microskin autograft.5,7 In this method the expansion ratio of the recipient site to the donor area can be greater than 10:1.7 Owing to the high utilization rate of the donor site and the simple procedure, microskin grafting has come to be one of the most important methods in China for the treatment of extensive burns with limited areas of normal skin.8 It has significantly reduced mortality and infectious morbidity in patients with major burns.8,9 Despite these favourable reports with microskin grafting, concerns about the poor cosmetic and functional results, especially in the joint area, remain problematic owing to the lack of dermis. To circumvent these problems associated with conventional microskin autografts, the allograft dermis, consisting of composite skin, has been utilized in order to improve cosmetic and functional results in adults.
In this paper, we report a co-graft of acellular ADM and autogenous microskin in a 6-yr-old child with major burns. The patient sustained a 72% TBSA burn, more than half being deep partial-thickness. Since 1996 our burns centre has gained considerable experience with the microskin autograft: since January 2006, 68 patients with major burns have had such microskin autografts. The general outcome of this experience is that the microskin autograft should be applied at the level of the fascia, which has a good blood supply. A fascial excision is therefore indicated for deep wounds in patients with 70% TBSA or more, unless very healthy deep dermis can be left.
No comments:
Post a Comment